







HAL haemorrhoidectomy and Recto-anal Repair (HAL-RAR)
Anatomy
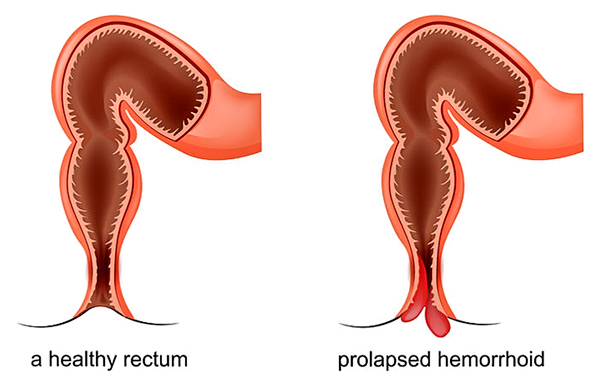
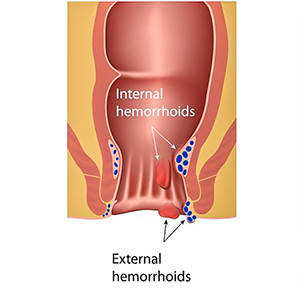
Haemorrhoids may be internal or external.
HAL haemorrhoidectomy
HAL haemorrhoidectomy is an ultrasound guided Haemorrhoidal Artery Ligation (HAL-RAR) haemorrhoidectomy. This is performed under general anaesthetic.
A specially designed piece of equipment with a built-in ultrasound is inserted into the anal canal. The artery supplying the haemorrhoids is located using the ultrasound.
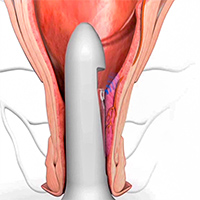
HAL Ultrasound
Once located, the artery is then sutured shut to reduce the blood entering the haemorrhoids tissue, thus reducing the tissue congestion.
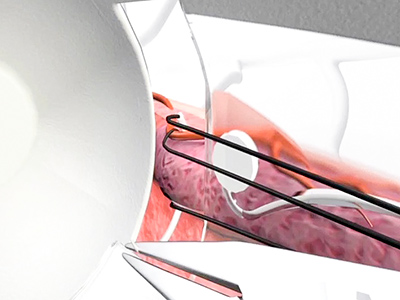
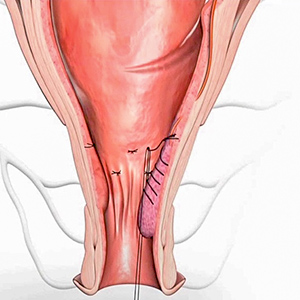
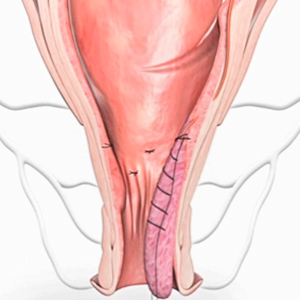
Surgery
The HAL haemorrhoidectomy is commonly performed together (at the same procedure) with the Recto Anal Repair. In this part of the procedure, the prolapsed haemorrhoid tissue is sutured (‘mucopexy’) and lifted upwards to its correct anatomical location.
No tissue is resected.
No tissue is resected.
The advantage of HAL over the conventional haemorrhoidectomy is the quicker recovery phase. There is significantly less pain post surgery and the patient is able to return to daily activities at an earlier date.
This procedure was first performed in Japan in 1995 and has been performed in Europe and North America now for a number of years with excellent results. 85% of patients have a complete resolution of their symptoms and over 90% are thoroughly pleased with the result even if there are some very minor residual symptoms.
This procedure was first performed in Japan in 1995 and has been performed in Europe and North America now for a number of years with excellent results. 85% of patients have a complete resolution of their symptoms and over 90% are thoroughly pleased with the result even if there are some very minor residual symptoms.
Complications
- Acute urinary retention—this is secondary to the discomfort. Co-existing prostate pathology is also an important factor.
- Minor bleeding.
- Feeling of incomplete emptying of the rectum. Patients may have the desire to empty their bowel 3–4 times a day but nothing happens when they get to the toilet. This sensation is temporary and tends to resolve after a few weeks.
- Other less common complications include: anal fissure, infection and anal skin tag formation.
Postoperative management
Mr Ahmad has instituted a ‘patients initiated postoperative analgesia regime’. Patients are assisted in managing their own analgesia (pain relief) whilst they are in the hospital. This is supported with written information sheets provided to the patient before the surgery. Using this regime, it facilitates a smoother recovery with less pain after the patients have been discharged.
Patients are discharged after opening their bowel in the hospital and after demonstrating proficiency of the postoperative analgesia regime.
Patients are contacted by the Post-operative Care Consultant in a few days after discharge.
Physical activities are encouraged except for lifting heavy weights and abdominal straining. There is to be no lifting for 2 weeks post-surgery and then 1–2 weeks of not lifting anything heavier than 5kg in weight which may be extended depending on the complexity of the surgery that had to be informed.
Please ask for further information.
Patients are discharged after opening their bowel in the hospital and after demonstrating proficiency of the postoperative analgesia regime.
Patients are contacted by the Post-operative Care Consultant in a few days after discharge.
Physical activities are encouraged except for lifting heavy weights and abdominal straining. There is to be no lifting for 2 weeks post-surgery and then 1–2 weeks of not lifting anything heavier than 5kg in weight which may be extended depending on the complexity of the surgery that had to be informed.
Please ask for further information.
Personal experience
Mr Ahmad was the first surgeon performing this procedure in Perth (since 2010) and has accumulated the most experience in this procedure.
There has been no mortality (death associated with the procedure), no return to the operating theatre to treat a complication, and with a temporal recurrence rate of less than 2%.
Most patients are able to return to work in the postoperative week 2 or 3.
There has been no mortality (death associated with the procedure), no return to the operating theatre to treat a complication, and with a temporal recurrence rate of less than 2%.
Most patients are able to return to work in the postoperative week 2 or 3.
Clinical Associate Professor Hairul Ahmad MBBS FRACS
Upper Gastrointestinal, Advanced Laparoscopic and General Surgery
Perth, Western Australia
Perth, Western Australia
Practice Details
Suite 12, Waikiki Specialist Centre,
221 Willmott Drive, Waikiki WA 6169
Please call (08) 9592 2298 for an appointment.
Fax: (08) 6314 1524
or email us
Office hours
9am–4pm Monday to Friday
Affiliations



© 2022 Perth General Surgery.
All Rights Reserved. Content and images on this website are subject to copyright.